Medical students often assume AI documentation tools simply transcribe conversations into text. The reality is far more sophisticated. Modern AI systems use advanced pipelines combining speech recognition, natural language processing, and large language models to create structured clinical notes that can match physician quality. This guide reveals how AI documentation actually works, what research shows about its effectiveness, and practical strategies to use it safely during your rotations while strengthening your clinical skills.
Table of Contents
- How AI Generates Medical Documentation
- Comparing AI-Generated Notes And Physician Notes
- Risks And Challenges With AI Medical Documentation
- Practical Tips For Medical Students Using AI Documentation During Rotations
- Enhance Your Clinical Documentation With MedCompanion Pro
- FAQs About AI For Medical Documentation
Key takeaways
| Point | Details |
|---|---|
| AI uses sophisticated technology | Speech recognition, NLP, and language models work together to transform conversations into structured clinical notes |
| Research validates effectiveness | Studies show AI notes match physician documentation in thoroughness while reducing time by up to 75% |
| Errors require vigilance | Hallucinations occur in about 1.47% of content, with 44% being clinically significant |
| Human oversight remains essential | Medical students must review and edit AI notes to maintain accuracy and develop documentation skills |
| Balanced adoption prevents burnout | Strategic AI use frees time for patient care and learning without eroding clinical judgment |
How AI generates medical documentation
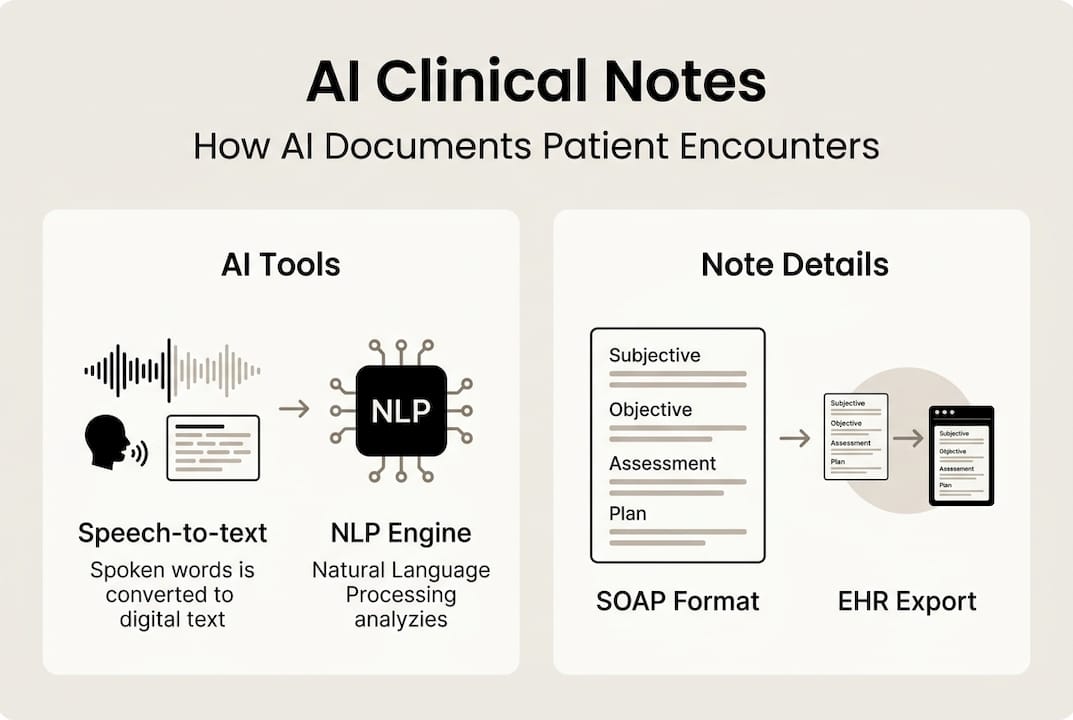
Understanding the technical foundation of AI medical documentation helps you use these tools effectively. The process involves multiple sophisticated steps working in concert. First, automatic speech recognition (ASR) captures spoken words during clinical encounters, converting audio into text with remarkable accuracy. Speaker diarization then identifies who said what, distinguishing between clinician and patient voices.
Next comes natural language processing, where the system performs named entity recognition to identify medical terms, symptoms, medications, and diagnoses. Intent classification determines the purpose of different conversation segments. The real magic happens when large language models like GPT-4 synthesize this information into structured clinical notes following standard formats.
Most systems generate SOAP notes: Subjective findings from patient history, Objective data from examinations, Assessment of the clinical picture, and Plan for treatment. Some platforms also produce specialty-specific formats. The entire pipeline processes a typical 15-minute encounter in under a minute, compared to the 10-15 minutes physicians traditionally spend on manual documentation.
AI clinical assistants integrate these notes directly into electronic health records, streamlining workflow. The technology operates passively during consultations, requiring no active input beyond starting the recording. This ambient approach lets you focus entirely on patient interaction rather than typing or writing.
Pro Tip: Always review the raw transcript before finalizing your note. Speech recognition errors in medical terminology can cascade through the entire documentation process, and catching them early prevents clinical mistakes.
The sophistication extends beyond simple transcription. Modern systems understand medical context, recognize common clinical patterns, and organize information logically. Research on AI scribe technology demonstrates how these capabilities transform documentation from a time burden into an efficient support tool.
Comparing AI-generated notes and physician notes
Peer-reviewed research provides concrete evidence about how AI documentation performs against traditional physician notes. A comprehensive benchmark study using the PDQI-9 quality framework evaluated both approaches across nine dimensions. The results challenge assumptions about AI limitations while highlighting areas requiring human expertise.
AI notes excelled in thoroughness and organization, capturing more clinical details and presenting them in clearer structures. Physicians maintained advantages in accuracy and succinctness, writing more precise notes without unnecessary information. Internal consistency scored similarly for both approaches. Time differences proved dramatic: GPT-4o generated notes in approximately 40 seconds versus 14.9 minutes for resident physicians.

| Quality Dimension | AI Notes | Physician Notes |
|---|---|---|
| Thoroughness | Higher score, captures more details | Good but sometimes misses minor points |
| Accuracy | Good but requires verification | Higher precision in clinical facts |
| Succinctness | Tends toward verbosity | More concise, focused content |
| Organization | Excellent structure and flow | Variable depending on individual style |
| Time to complete | 40 seconds average | 14.9 minutes average |
| Internal consistency | Strong logical coherence | Strong logical coherence |
AI documentation advantages include:
- Consistent formatting across all encounters
- Comprehensive capture of discussed topics
- Immediate availability after patient visits
- Reduced documentation burden and burnout risk
- Standardized terminology and structure
Physician documentation strengths include:
- Superior clinical judgment in complex cases
- Better discrimination of relevant versus irrelevant details
- Contextual understanding from longitudinal patient relationships
- Nuanced interpretation of ambiguous findings
- Personalized communication style
For medical students, these findings suggest AI serves best as a drafting tool rather than final product. The technology accelerates the documentation process while you maintain responsibility for clinical accuracy. AI clinical assistants complement your developing skills without replacing the critical thinking required for excellent patient care.
The implications for learning are significant. Using AI notes as starting points lets you focus on clinical reasoning rather than mechanical transcription. You can compare your assessment with the AI's interpretation, identifying gaps in your knowledge or documentation approach. This comparative process strengthens both clinical judgment and communication skills.
Risks and challenges with AI medical documentation
Every technology carries limitations, and AI documentation presents specific risks requiring awareness and mitigation strategies. Hallucination rates average around 1.47% of generated content, with 44% of these errors significant enough to impact diagnosis or treatment decisions. Understanding error patterns helps you catch mistakes before they affect patient care.
Common AI documentation errors include:
- Fabrications where the system invents details not mentioned in the conversation
- Negation mistakes that reverse the meaning of clinical findings
- Causality errors linking unrelated symptoms or conditions incorrectly
- Omissions of critical information, especially in assessment and plan sections
- Medication dosage or frequency inaccuracies
- Misattribution of symptoms between different body systems
Certain clinical situations increase error probability. Noisy environments with background conversations confuse speaker diarization. Accented speech or rapid talking challenges speech recognition accuracy. Complex cases involving multiple diagnoses or rare conditions strain the AI's pattern recognition. Edge case risks multiply when encounters deviate from typical presentations the system trained on.
Over-reliance poses another significant concern. Medical students developing documentation skills need hands-on practice writing notes from scratch. Exclusively using AI-generated drafts can prevent you from internalizing proper documentation structure and clinical reasoning flow. The convenience of automated notes might discourage the deliberate practice necessary for expertise development.
Pro Tip: Create a personal QA checklist focusing on high-risk sections like Assessment and Plan. Before finalizing any AI note, verify medication details, check that diagnoses match your clinical impression, and confirm the plan aligns with your intended treatment approach.
Privacy considerations deserve attention as well. Patients must provide explicit consent before AI systems record their conversations. Some individuals feel uncomfortable with automated documentation, preferring traditional methods. Respecting these preferences maintains trust and adheres to ethical standards.
The assessment and plan sections contain the highest concentration of errors because they require clinical judgment beyond simple transcription. AI systems struggle with the nuanced reasoning connecting symptoms to diagnoses and diagnoses to treatment decisions. Always scrutinize these sections carefully, treating them as suggestions requiring validation rather than authoritative conclusions.
Accessing raw transcripts when possible provides another safety layer. Reviewing what the AI actually heard lets you identify speech recognition errors before they propagate through the note. Many platforms offer this feature specifically for quality assurance purposes. AI clinical assistants that provide transcript access give you greater control over documentation accuracy.
Practical tips for medical students using AI documentation during rotations
Successfully integrating AI documentation into your clinical workflow requires deliberate strategies balancing efficiency with learning. Follow this systematic approach to maximize benefits while minimizing risks:
- Draft your own assessment and plan before reviewing the AI note, preserving your clinical reasoning development
- Compare your draft with the AI version, noting differences in interpretation or completeness
- Evaluate the AI note using PDQI-9 criteria focusing on accuracy, thoroughness, and succinctness
- Edit the assessment and plan sections first, as these contain the highest error rates
- Verify all medication names, dosages, and frequencies against your prescription intentions
- Cross-check diagnoses with your clinical impression and examination findings
- Review the subjective and objective sections for omissions or fabrications
- Finalize the note only after confirming it accurately represents the encounter
Environment and consent best practices include:
- Conduct encounters in quiet rooms when using AI documentation to improve speech recognition
- Obtain explicit verbal consent from patients before starting AI recording
- Explain how the technology works and what happens to the data
- Offer alternative documentation methods for patients who decline
- Position recording devices to minimize background noise interference
- Speak clearly and avoid medical jargon when addressing patients directly
| Documentation Method | Average Time | Quality Score | Learning Value | | --- | --- | --- | | | Manual notes only | 14.9 minutes | 8.2/10 | High | | AI draft with review | 3.7 minutes | 8.1/10 | Medium-High | | AI with minimal review | 1.2 minutes | 6.8/10 | Low |
Maintaining an error log strengthens your quality assurance process. Document every AI mistake you catch, categorizing by error type and clinical context. This personal database reveals patterns in where the technology struggles, making you more efficient at spotting problems. After a few weeks, you'll develop intuition for which note sections require extra scrutiny.
Balanced adoption means using AI strategically rather than universally. Consider drafting complex or unusual cases manually to reinforce your documentation skills. Reserve AI assistance for routine encounters where time savings matter most. This mixed approach preserves learning opportunities while reducing overall documentation burden.
Research demonstrates that thoughtful AI adoption reduces documentation time by up to 75% without compromising clinical judgment. The key lies in maintaining active engagement with the documentation process rather than passive acceptance of automated output. Best practices for ambient scribing emphasize human oversight as the essential safeguard ensuring patient safety.
Time saved through AI documentation creates opportunities for deeper patient engagement, additional study, or self-care preventing burnout. Medical students who adopt these tools strategically report better work-life balance without sacrificing educational quality. The technology serves you best when it amplifies your capabilities rather than replacing your clinical thinking.
Enhance your clinical documentation with MedCompanion Pro
Now that you understand how to use AI documentation effectively, consider a platform designed specifically for medical students and interns. MedCompanion Pro combines ambient scribing with comprehensive clinical support tools tailored to rotation workflows. The platform supports French, Romanian, English, and German, making it ideal for international medical education settings.
Key features include guided anamnesis that structures your patient interviews, real-time clinical reasoning support, and automatic result extraction from investigations. The system generates notes in multiple formats including PDF and DOCX, integrating seamlessly with electronic health records. Differential diagnosis suggestions help you consider alternatives while developing clinical judgment.
What sets MedCompanion Pro apart is its focus on learning alongside efficiency. Case simulations and quizzes reinforce concepts while you document real patients. The medical vocabulary encyclopedia clarifies terminology as you encounter it. GDPR compliance and end-to-end encryption protect patient privacy throughout the documentation process.
Pro Tip: Start with MedCompanion Pro during your next rotation to experience how AI documentation preserves learning while reducing time pressure. The platform's review features encourage active engagement with generated notes rather than passive acceptance.
Visit MedCompanion Pro to explore how AI can transform your clinical documentation experience while supporting your educational development. The combination of time savings and structured learning support makes rotations more manageable and educational outcomes stronger.
FAQs about AI for medical documentation
What safeguards ensure AI notes don't contain harmful errors?
Multiple safeguards protect against harmful errors in AI documentation. Human review remains mandatory before finalizing any note, with physicians or students verifying accuracy against their clinical assessment. Quality frameworks like PDQI-9 provide structured evaluation criteria. Many platforms flag uncertain or low-confidence sections for extra scrutiny. MedCompanion Pro incorporates review workflows that prompt verification of high-risk content before finalization.
Can AI documentation adapt to different medical specialties during rotations?
Yes, modern AI systems adapt to specialty-specific documentation requirements. The technology learns different note structures for cardiology, pediatrics, surgery, and other fields. Some platforms let you select specialty templates that guide the AI toward appropriate formatting and terminology. Training on diverse medical literature enables recognition of specialty-specific patterns and language. Performance varies by specialty, with primary care and general medicine showing strongest results currently.
How much time can AI realistically save medical students on documentation?
Research shows AI documentation reduces time from an average of 14.9 minutes per note to approximately 3-4 minutes including review time. This represents roughly 75% time savings compared to manual documentation. The exact amount depends on encounter complexity, your review thoroughness, and AI system quality. Simple follow-up visits save more time than complex new patient evaluations. Most students report reclaiming 1-2 hours daily when using AI documentation consistently.
Does using AI notes affect learning and clinical skills development?
AI documentation impacts learning positively when used strategically but can hinder skill development if over-relied upon. Students who draft their own assessment before reviewing AI output maintain strong clinical reasoning skills. Those who passively accept AI notes without critical evaluation show slower documentation skill growth. The key is active engagement, treating AI as a collaborative tool rather than replacement for thinking. Comparing your reasoning with AI suggestions often reveals knowledge gaps worth addressing.
What privacy considerations should students know when using AI scribing tools?
Patient consent is legally and ethically required before recording clinical encounters for AI documentation. You must explain how the technology works, what data gets stored, and who accesses it. HIPAA compliance in the US and GDPR in Europe mandate strict data protection standards. Choose platforms with end-to-end encryption and clear data retention policies. Never use consumer AI tools like ChatGPT for clinical documentation, as they lack necessary security safeguards. MedCompanion Pro meets healthcare privacy standards with GDPR compliance and encrypted data handling.